

By Ellie Atkins
As a manager and safeguarding lead for a social work team in Manchester, I work with people experiencing severe multi-exclusion homelessness.
In this article, I will explore the context in which people’s struggles appear and suggest what we can do as social workers to improve the lives of some of the most misunderstood people in our society.
Cast your mind back to the Covid pandemic when ‘The Everybody In’ initiative provided hotels for people to come indoors for safety, backed by financial investment, legal frameworks and political will.
Why refuse shelter?
Despite this humanitarian response, some people refused to come indoors or behaved in such a way they could not stay in.
Why would you ‘choose’ to remain on the streets during a pandemic, when safety through hotels was being provided?”
In Manchester, this group of people met the three-tier threshold for a safeguarding enquiry under the Care Act 2014: they had needs for care and support, they were neglecting their care for self and their basic needs and were behaving in ways in which they could not be protected or indeed protect themselves.
With professional curiosity and compassionate enquiry to understand the ‘why’, alongside a research project, it became clear that the people remaining on the streets were likely to have hidden disabilities and differences that affected their executive functioning.
About executive function
Our executive functioning, which is located the frontal lobes of our brain, allows us to plan, problem-solve, inhibit our behaviour and emotions, make goals, see them through and have the ability to act out our wishes and be who we want to be.
When our executive functions are compromised or impaired in some way, this is called executive dysfunction. It can be hard to spot and slippery, because it changes, depending on the environmental, emotional and social context we find ourselves in.
I would suggest using the wheel pictured below, which sets out eight dimensions of executive functioning, to help with understanding the concept.
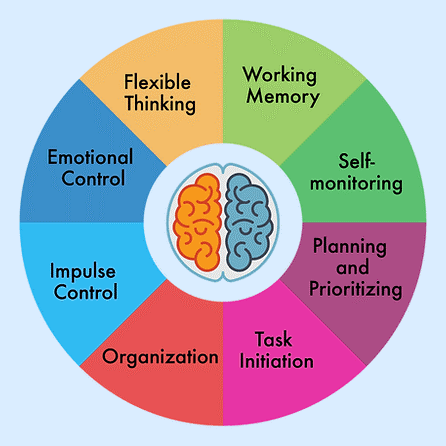
A wheel illustrating the different aspects of executive functioning
Some conditions are well evidenced to affect out executive functioning, such as acquired brain injury, foetal alcohol syndrome disorder, complex post-traumatic stress disorder, attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD) and other forms of neurodivergence.
A 2022 study found that 92% of 115 people using a homelessness service had experienced trauma (Irving & Harding, 2022), whereas 48% of homeless respondents to a 2012 piece of research had acquired brain injuries (Oddy et al, 2012). This means that this group is much more likely to experience executive dysfunction than the wider population.
Focusing on safety
We can then move the power dynamic from, ‘What’s wrong with you?’, to, ‘What do you need?’, placing the onus on us as social workers to support the person to optimise their executive functioning before the Mental Capacity Act 2005 is considered or engaged in cases of significant self-neglect.
You see, executive functioning can be stabilised and optimised when we meet the non-negotiable human need to feel safe: safe in body, safe in where we live, safe in who is around us and safe in the way that people work with us.
This truly strengths-based approach, underpinned by relational social work, the power of human connection, kindness and empathy, can mean everything and costs nothing.
Beryl’s story
Can I introduce you to a lady called Beryl? Beryl will show you how we can use the Care Act, our assessments, support planning and safeguarding, alongside the executive functioning wheel and relational social work, to enable people to have better outcomes and better lives.
Beryl had been known to our team for 10 years, as a lady with chronic and dependent alcohol addiction who said she did not want to work with services or receive help with her drinking.
When I moved our focus from her alcohol addiction and homelessness, during the Everyone In initiative, and tried to understand ‘why’ she would behave in this way, the context in which her struggles appeared started to become unveiled.
I used the Care Act provision to override a refusal of assessment when someone is experiencing, or at risk of, abuse or neglect, and a team around the person approach, to gain an understanding of Beryl’s life story.
Understanding the ‘why’
Beryl had experienced adverse childhood experiences and significant trauma; she lost her baby in a car accident, she experienced a head injury and later witnessed her partner being murdered. Beryl drank all day, every day, because she was too scared to stop.
Beryl’s behaviour became so distressing to herself and the wider public that we had to use police powers under section 136 of the Mental Health Act 1983 to take her to a place of safety and then placed her under section 2 of the MHA for a period of assessment. These decisions are not taken lightly.
Beryl was then moved to section 3 of the MHA and responded to treatment.
She states that this was the first time, in as long as she could remember, that her mind became safe and calm, enabling her to communicate in a way she wished to. It was during this time that she was diagnosed with ADHD, post-traumatic stress disorder and an acquired brain injury.
Whilst ‘labels’ may not always be helpful, Beryl had lived with hidden disabilities, with limited quality of life, believing that she was a moral failure for her alcohol dependency.
Being who you want to be
Beryl now lives in supported accommodation, she attends Alcohol Anonymous and supports other peers in their own recovery from addiction. Beryl states that, for the first time, she has the ability and capacity to be who she wants to be.
If Beryl’s story resonates, please find out more by watching these videos about her.
Her story reminds me of what Desmond Tutu once said:
There comes a point where we need to stop just pulling people out of the river. We need to go upstream and find out why they’re falling in.”
Ellie Atkins is manager and safeguarding lead for the entrenched rough sleeper social work team at Manchester City Council
References and further reading
Bramley, G et al (2015) Hard Edges: Mapping severe and multiple disadvantage, England Lankelly Chase Foundation
Grant, S et al (2016) Experiences of Homelessness and Brain Injury Sheffield Hallam University
Irving, A & Harding, J (2022) The Prevalence of Trauma among People who have Experienced Homelessness in England Oasis Community Housing
FEANTSA (2017) Recognising the link between trauma and homelessness
Oddy, M, Moir, J, Fortescue, D, & Chadwick, S (2012) The prevalence of traumatic brain injury in the homeless community in a UK city Brain Injury, 26(9), 1058–1064


 Bournemouth, Christchurch and Poole
Bournemouth, Christchurch and Poole  Hampshire County Council
Hampshire County Council  Oxfordshire County Council
Oxfordshire County Council  South Gloucestershire Council
South Gloucestershire Council  Wokingham Borough Council
Wokingham Borough Council  Webinar: building a practice framework with the influence of practitioner voice
Webinar: building a practice framework with the influence of practitioner voice  ‘They don’t have to retell their story’: building long-lasting relationships with children and young people
‘They don’t have to retell their story’: building long-lasting relationships with children and young people  Podcast: returning to social work after becoming a first-time parent
Podcast: returning to social work after becoming a first-time parent  How managers are inspiring social workers to progress in their careers
How managers are inspiring social workers to progress in their careers  Workforce Insights – showcasing a selection of the sector’s top recruiters
Workforce Insights – showcasing a selection of the sector’s top recruiters 



 Facebook
Facebook X
X LinkedIn
LinkedIn Instagram
Instagram
Thank you so much-this is a really inspiring article. I love the focus on the non negotiable human needs too
The latent theme running through the rise of neuroscience and neuro-diversity is the reflexive knowledge that such ideas are seated in the Keirkegaardian notions of abandonment.
Executive brain function is also impacted by indifference and systemic invalidation and the additional societal attitudinal injury to an already injurious life position that is so readily perpetuated and equally easily changed with an ordinary expectation of kindness and compassion based work.
As ever though the process of re-conceptualisation of the issues raised in this article must also balance the notions of an implicit social and personal inadequacy with the structural inadequacies of a failure in how access to accommodation and housing remains the persistent problem.
Keirkegaardian notions are also and inevitably based on a white protestant world view; that equity groups like Waterland, a Danish Group,are now funding primary care to a huge extent and with a regional if not national market share, and this too must also be weighed in the mix.
Homelessness, has always been a cash cow and the repeated policy attempts to tame the financial exploitation of this have to date failed, and miserably so.
Manchester has a good historical track record in altering perception and practice going back decades ~ I am thinking of the Peterloo Project and I would hope that this work, acknowledging the structural and financial issues, gains credence. The idea and practice of therapeutic communities while old hat for old dogs like me does actually work.
For more on such see Peter Rollins and Julie Reshe.
This said, our own learning mustn’t ignore the case for ‘conviviality’ made within the industry in 1997 ~ when attempts were made through a broader alignment of resources targeted at the prevention of the collapse of families and communities, and literally on a street-street level (the super output area’s) through life-long learning and family centres. David Blunketts, time as SofS for Education was successful in the radicalisation of a fresh approach to such.
Let’s see if Bridget Philipson can do something similar. The mind set here must be though harnessed to the correct economic drivers and if connections are made to the idea of economic transitivity* aimed specifically at women and children then the impact could be truly mind blowing.
*economic transitivity simply states that by bringing the health needs of marginal groups upto the levels of the wider population brings benefits to both ~ without health and welfare economic drivers, as signifiers for change, at population level the advantages of the neurosciences will not gain traction*
this article captures the essence of tragic lives
however it papers overs the lack of kindness and compassion shown by families and wider society to those who struggle.
prisons can also perpetuate the trauma and some ‘so called’professionals use big words to explain simple concepts.
we can and should do more, we have the resources, it’s the little acts of kindness that help people not forced interventions by statutory services
interesting points, gill ~ yet, when ‘we’ have looked at this many initiatives add to the permanence of homelessness ratherthan addressing it see Josh Burraway, Intoxicating Ethics for a critical take on the services and issues.